

You can find my most recent commentaries on the Junior Doctors’ crisis as it unfolds in 2008 by following this link.
Ok, MTAS. What to say about the Medical Training Application Service? Context first, I think and then up close and personal with the mad, brutal, arbitrary shambles of the computerised system tomorrow. (I want you to think of mindless zombies walking blindly through the streets, picking up people, shaking them about a bit, discarding some like broken dolls but letting others crash-land wherever their bad luck takes them. That is MTAS.)The problem with most commentary on MTAS is that much of it is written by people who are directly involved and – frankly – deeply traumatised by the experience. I’m trying to keep the purple prose to a minimum but every now and again an image, like the zombies above, just takes over.
The other problem with commenting on MTAS is that those who aren’t directly involved can rarely believe what they are reading, the whole thing is so shambolic, brutal and wasteful.
We’ve already established that, for reasons of its own, the government has decided to squash 9-12 years’ specialist medical training into 5 years, discarding about 20% of the doctors who are suitably qualified in the process. Let’s look at the hoops we are putting them through before we discard them.
The thing that is mad about MTAS is that it is a geographical form of russian roulette.
Doctors are not allowed to apply to local hospitals or to specific NHS Trusts. Oh no. Doctors part way through their specialist training are being forced to make four applications (neither more nor less) to four different parts of the country. When I tell you that the whole of Scotland is one deanery, Wales is another, Kent-Surrey-Sussex-London is a third, and that there are 12 across the rest of England, you’ll appreciate that the chances that a doctor will have to drag her partner three quarters of the way across the country are spectacularly high. Even if she gets a job in her own deanery, the deaneries are huge and there is no guarantee that she’ll be working within even two hours of where she lives. And why? The hospital she lives half a dozen miles from will be recruiting for doctors with just her skills and aptitudes, but the anononymisation of the forms mean that location is not taken into account when offering interviews. I dislike the phrase political correctness gone mad, but this is fairness gone mad.
Of course, every NHS hospital in the country employs junior doctors in various stages of specialist training. There are roughly 28,000 of them. Most of them them are in relationships, either with other health professionals or with non-medics. Many of them have children. All of them have friends. All of them know and understand the workings and foibles of their particular hospitals, and of the population they serve.
I know its obvious to you, and I apologise for New Labouring the point, but you are not a politician so you do actually understand these things.
Come August, every hospital in the country will still need doctors in various stages of specialist training. It is clearly preferable to employ suitably qualified people who are local because they will not be distracted by moving and their partners will be established in their own careers or happily embedded in a network of friendships and family life. It is useful for everyone if the doctors have established relationships with hospital and other health-care staff. Happy doctors make for better patient care.
Yes. I’d have thought that was obvious too, but then I am not a politician.
Instead of letting doctors apply to individual hospitals or to specific local NHS trusts, the government has decided that a Great National Clearing Scheme is better. This shows all the signs of being designed to solve a problem we no longer have. A Great National Clearing Scheme would help to make sure that there were enough doctors in the really unpopular hospitals if there weren’t enough doctors to go round. But there are more than enough doctors to go round, so a Great National Clearing Scheme confers no advantages at all.
The thing that is brutal about MTAS is that it is a professional form of russian roulette.
This one has nasty bullets, because for the one in four applicants hit by one, then that’s it. If they didn’t get a specialist training post this time, then they are explicitly prevented from applying again. No job in the NHS for them. No more specialist training in the UK either. They had the one chance to get a specialist training contract and those chances were handed out in February. Thank you and goodbye. Nice stethoscope, shame about the university debts. (Doctors pay about £30,000 for their education, and most of them leave university with a certificate and a letter from the bank asking them to start repaying it now please).
This is the bit that most members of the public who comment on blogs and on-line newspaper forums simply don’t believe. I cannnot blame them for assuming that the doctors are exaggerating because it really does beggar belief. It’s true though. This is a one-chance-only event for specialist doctors.
The thing that is arbitrary about MTAS is that it is a game of poker where the deck’s been fixed.
Theoretically it should be fair, but the way that the government has applied it has actually invalidated the whole system. That was not my opinion at the start of the whole debacle. That was what I discovered when I waded through the academic research on the subject. I’ll go into the details of the process itself tomorrow, and tell you what I found out from the research papers on the best ways to assess the ability of candidates to do the job they are applying for. As a taster, I’ll tell you that the method that is being used scores about 3 on a scale of 0-10.
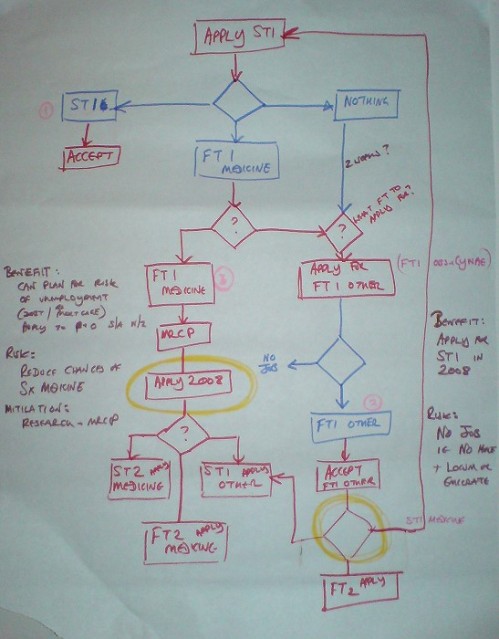
In the meantime, to show you how tortuous the whole thing is for those entering the system at the bottom, here is a picture.
A patients’ guide to Modernising Medical Careers Part 1 explains why are now “too many” doctors in specialist training and how the government has decided to cut their numbers.
Part 2 looks at the way MTAS forces doctors to relocate at random around the country, uprooting their partners and families in the process.
Part 3 considers the academic research on recuitment and assessment methods and discovers that the Self Assessment Competency Questionaires have been invalidated by the way in which they have been introducted.
Part 4 considers the debt we owe to the overseas-trained doctors and how we are repaying it. With a kick in the teeth, basically.

My son has been trying to explain why he might be going off to the antipodes. I don’t mind, I’ve long fancied a treck around Australia and Diving off the West Coast. But what a bloody waste. He’s a good doctor and has been shortlisted but is still so frustrated! I know the other political parties are probably as bad and keeping very quiet, but perhaps now people will wake up to what the party of envy (Labour) are really about. Whilst putting all these doctors out of the medicine, I don’t suppose this tosspot government will have the good grace to cancel the student debts still to be paid off??
You’ve done it again! Fantastic way of describing how junior docs are in the midst of the national jobs lottery! Had been eagerly waiting all morning to read this! Don’t keep us waiting too long for the third instalment…
Thanks for commenting Vincent. One of the reasons I’m writing these pieces is to explain it to those – like myself – who are peripherally involved and who struggle to work out why the rug has suddenly been pulled out from underneath our own favourite medics. Your point about the student debts just underlines the cynical hypocrisy of the whole thing. I admire the good grace that the two of you are showing in these circumstances. Hell, I admire the good grace of the whole profession. I wish your son the best of luck, but these days I don’t know if that means “I hope he gets a job here” or if it means “I hope he manages to escape”.
Alexandra, thanks for your enthusiasm. The third installment will be out tomorrow I promise.
Aphra.
Are you going to do a post about the specific implementation issues too? (eg mad timetable, litany of errors, crashing website etc).
I would even volunteer to collect up examples and data for you, if you like, and if you then put it together into an elegant post. I did consider doing what you’re doing, but my blog is non-political, and also I don’t know that I’d have the sustained energy to do the subject justice, and there are enough half-assed versions out there already. But I’m glad you’re doing it.
I’m pushed for time (though you wouldn’t believe it – the amount of time I spend on this).
I’m trying to stick to subjects that other people are not covering, or to perspectives that other people are not looking at. I assumed that there is a lot out there which is pretty accessible about the implementation issues and recent events like the West Midlands Surgeons, (may their scalpels always stay sharp) and the so-called Review by the government.
I do glance on the cock-ups. But not in my own words. Have you seen: https://aphrabehn.wordpress.com/mmc-and-mtas/mmc-and-mtas-in-private-real-stories-real-doctors/
This isn’t actually a political blog. It is just that Tony Blair is a s**t.
Aphra.
I just had to add that the graphical representation is a wonderful piece of art. Great site and thanks for helping create more debate over such an important issue. Thanks again, Michelle
Thank you Michelle. It is colour coded, an’ has dates an’ evvryfink.
Aphra.
Pt 1 – superb – thank you
Pt 2 – text – very clear – well done
Pt 2 diagram – obscure, incomprehensible, communicates nothing at all, except perhaps to the in-crowd (ie exactly what you set out NOT to do).
Perhaps you are getting tired. I don’t blame you. Part 1 is achievement enough. Big disappointment, Pt 2, nevertheless.
The diagram was personal, really; a decision-path I worked out with the one Mums4Medics calls “my” doctor to help him work his way through his own thought processes. It has been overtaken by events again and again and again. I posted it here to make the point that the MTAS process is, as you rightly say, obscure and incomprehensible. I guess it illustrates that point perfectly.
I am glad the text was helpful.
I wish you and yours luck through this whole sorry mess.
Aphra.